Disorderly Conduct
 Originally published in the Washington Post Magazine: May 28, 2000
Originally published in the Washington Post Magazine: May 28, 2000
In the case of Margaret Walters v. Downey Communications, a pregnancy discrimination lawsuit became a nasty legal slugfest for a revolving cast of combative lawyers
For Margaret Walters, it all began with what she wore. She studied her figure in the mirror and felt pleased that the navy-blue pants with the tattered lining still fit, even now, in her second trimester of pregnancy. Her husband, Steve, was at work; 2 1/2-year-old Elizabeth was at preschool. Margaret was grateful for the stillness in the house and the chance to collect her thoughts before the job interview.
For the last year Walters had been restless as an account executive with a marketing company north of Baltimore. When she'd heard from a co-worker about an opening at another marketing research company in Bethesda in early May 1994, she seized the chance. As she drove from her house in Arlington to the offices of Marketing & Management Information Inc., she felt a twinge of nervousness but was hopeful that this interview might be the first step toward a welcome change in her life.
In the joint reception area of MMI and its sister company, Downey Communications Inc., Walters shook hands with Harvey Richmond, vice president of marketing and sales.
From the deposition of Harvey Richmond, 3/2/98, the U.S. Equal Employment Opportunity Commission v. Downey Communications Inc.:
Q: Did you believe she was pregnant after her first interview?
Richmond: It never crossed my mind.
Q: Was she wearing maternity clothes at her first interview?
Richmond: I don't think so.
The interview went well, and Walters was invited back a few weeks later. This time, there were more introductions and an enjoyable conversation with Ed Downey, who co-owned DCI/MMI with his wife, Loretta. Over lunch, Walters, Richmond and several MMI employees talked about a variety of things, including her playing on the company softball team. When she left, she felt certain the job was hers.
From the deposition of Edward M. Downey, 3/25/98:
Q: Is it fair to say that in your opinion anybody would have been able to tell that she was pregnant?
Mr. Grayson [for the defense]: Objection; asked and answered twice now.
The Witness: I think anybody could see that she was pregnant if they were conscious in observing the fact.
By Mr. Hutter [Dana Hutter, attorney for the EEOC]:
Q: Did you ask her when she was due?
Mr. Grayson: I want to go back to the previous question. I think that I'm going to object also because the question calls for speculation on the part of the witness. I don't understand how you think that this witness can say whether everyone would know that she is pregnant. Are we talking about my three-year-old daughter? Are we talking about the Pope? Who are we talking about here?
The Witness: As I told you, I did not discuss her pregnancy. I didn't think it was appropriate.
About a week after the second round of interviews, Walters received a call from Richmond, offering her the position of manager of client services.
Letter from Harvey Richmond, 6/3/94:
Dear Margaret:
Confirming our recent discussion, Marketing and Management Information, Inc. is pleased to offer you the position of Manager, Client Services. This is a key function at our young, rapidly growing company. Margaret, we believe that you have the experience, maturity and people skills to be a great asset to our company. We also believe that we offer you the opportunity for a lucrative and professionally satisfying long term career.
The offer was thrilling to Walters, and she called Richmond back to accept, agreeing on a start date of July 1. At that point she mentioned to him that she was pregnant and due in October. Walters noticed a pause on the line, then Richmond said, "I'll need to work that issue internally." The conversation ended cordially, yet this last moment of awkwardness etched itself uncomfortably in Walters's mind.
After writing a formal acceptance letter, Walters placed it in an envelope and put it on the stack of outgoing mail.
She never mailed it. That same afternoon Richmond called back. "I'm sorry," he told her, "but we can no longer offer you the position. The job specs have changed."
Walters was stunned. Over the span of a few hours she had accepted and already lost a new job.
Letter from Harvey Richmond, 6/7/94:
Dear Margaret:
As we discussed earlier today, Marketing and Management has entered into an agreement to purchase a new data base operating system. This acquisition is a very major investment and expansion for our company. As such, it will significantly change the requirement of the position that we have discussed with you . . . In light of these new and unexpected developments we have postponed our hiring decision for this position . . .
By evening, Walters had gone from shock to outrage. She was convinced that the company had concocted a version of events in order to "unhire" her. On June 9, 1994, she filed a claim of pregnancy discrimination against DCI under Title VII of the Civil Rights Act of 1964 jointly with the Maryland Commission on Human Relations and the federal EEOC.
What followed was nearly five years of protracted and costly civil action, amid a bizarre barrage of legal taunts and threats. For reasons that are still unclear even to the participants, a convoluted set of agendas overtook this case. What began as a personal disappointment -- a person is offered a job, then the offer is withdrawn -- became a free-for-all among lawyers that, in the words of U.S. District Judge Frederic N. Smalkin, was "over-lawyered and overpapered to an extent the likes of which I have not seen in 20 years' experience in this district." Perhaps the best way to follow the developments of the case is through the paper trail that litters the narrative of Margaret Walters v. the Downeys.
Ed and Loretta Downey run an informal company. Wandering freely about the offices are three springer spaniels, Oliver, Kelly and Chelsea, whose "business cards" read Official Greeter, Chief of Security and Top Dog, respectively. Policies and procedures are not always written down, and job descriptions are loosely defined, sometimes overlapping.
In May 1994, when Walters came for her interview, DCI/MMI had about 70 employees, a relatively small company in the marketplace. The company was attempting to purchase a new processing system -- at $250,000 -- that would be the biggest single investment it had ever made. Although the new system would give the Downeys a chance to be more competitive against their larger rivals, in the short run it was a terrifying plunge. Before the deal was finalized, Pat Flannery, MMI's executive vice president, was often on the phone until midnight in negotiations.
This was not the only unnerving issue facing the Downeys. Loretta did not meet Walters during the second interview because she was at Sibley Hospital, where she had learned that the lump in her breast was cancerous. When the good news came through about the database agreement, the entire office celebrated -- but without Loretta. She was undergoing tests and sifting through the complex decisions she would need to make regarding treatment.
The Downeys contend that Harvey Richmond had been out of the loop regarding the new system. Once he was debriefed, he could see that the requirements for manager of client services would drastically increase. The position might be negated entirely. So he decided to postpone hiring Walters.
Deposition of Loretta Downey, 3/24/98:
Mr. Hutter: When did you first learn that Margaret Walters had sought a position with MMI?
Mr. Grayson: I would like to note for the record it is now 3:34 in the afternoon. This witness has been testifying since 9:00 this morning. This is the first question that you have asked regarding Walters or the discrimination charges in this case.
Mr. Hutter: Can you answer the question?
The Witness: When she took legal action against DCI.
To the Downeys, the charge of discrimination was ludicrous -- DCI was co-owned by a woman after all. They had had several pregnant employees in the past, they say, and had worked hard to accommodate their needs and schedules, even providing generous leave time.
Two weeks after filing her suit, Walters's phone rang. It was Alan Grayson, who identified himself as the attorney representing the Downeys. Walters found his manner threatening and adversarial. He left her with the sense that if she didn't back down and withdraw the claim, they would have no qualms about making life difficult for her.
Instead of backing down, however, Walters signed a retainer with attorney Chet Levitt, of Jacobs, Jacobs & Farber in Rockville.
Despite their insistence that they had done nothing wrong, the Downeys wanted a quick end to the matter, and they authorized settlement discussions between Levitt and Grayson's associate, Fred A. Cohen. A hostile exchange of correspondence set the tone for years to come.
Letter from Fred Cohen, 7/8/94:
Dear Mr. Levitt: I write to respond to your settlement demand dated July 6, 1994. I hope that I received the entire letter. After all, the portion of the letter that I received did not contain a demand that Downey Communications, Inc. ("Downey") transfer to Ms. Walters the title to the wizard's castle in "The Wizard of Oz."
If Ms. Walters desires to accept the settlement offer dated June 27, 1994, the offer will remain open until 5:00 p.m. on Monday, July 11, 1994. You can be assured that Downey will vigorously defend itself if the offer is not accepted . . .
For the next several months, Walters spent much of her time making phone calls to nudge things forward. Each time she called the Maryland human relations commission to find out the status of her case, she was told that the supervisor with whom she was supposed to communicate was "on vacation." Walters had recently been laid off from her job due to company cutbacks. She had interviewed with two other companies while very noticeably pregnant and had gotten nowhere. In October, Walters gave birth to a girl, whom she and Steve named Jackie.
With Walters unemployed and the arrival of a new baby, money was tight. Steve urged her to come to some agreement with the Downeys and take whatever money they offered her. Frustrated by the lack of progress on her case, she prodded her lawyers yet again for action.
By November, settlement correspondence had fluttered back and forth between Levitt and Cohen, who finally agreed upon the sum of $3,750. Walters says her attorneys were never authorized to accept such an offer without her approval. The Downeys contended that there had been a solid verbal agreement and accused her of reneging. Breach of settlement, they knew, was a violation of the law.
At this point Walters decided to fire Chet Levitt and his law firm, frustrated with their lack of progress. Then another person arose to champion Walters's cause.
Elaine Sykes has been an investigator for the Maryland Commission on Human Relations for 11 years. She is also a Baptist minister. Sykes believes the investigator job's primary necessity is common sense, although she carries a copy of the Code of Maryland Regulations with her at all times. She is not someone who scares easily. Six months after the original charges were filed, the commission assigned Sykes to Walters's case. She told Walters that settlement was an option, but the charges would have to be dropped. Walters was already appalled at the personal and financial costs of filing the suit, but she was not willing to back down.
Sykes went to work. She sent DCI a request for information that listed nine categories of documentation to be submitted within the week. Cohen replied with what became DCI's first line of defense: that Walters had sued the wrong company.
Letter from Fred Cohen, 12/15/94:
Dear Ms. Sykes:
. . . DCI does not own MMI or any of MMI's stock; MMI does not own DCI or any of DCI's stock; the Complainant here, Margaret Walters, never applied for, or was offered, employment with DCI; Ms. Walters applied for a position with MMI, as her experience related to sales and marketing data . . . It follows that there can be no finding that DCI discriminated against Ms. Walters, and therefore the above charge must be dismissed . . .
At Sykes's urging, Walters then filed an amended charge of discrimination including MMI as a respondent. Cohen countered that it had been filed six days beyond the six-month statute of limitations. He accused the commission of illicitly backdating the claim. In a letter to Cohen, Elaine Sykes quoted from the statutes themselves: "All amendments shall relate back to the original filing date." She then slapped the company with a subpoena, now demanding 21 categories of documents.
Letter from Fred Cohen, 3/14/95:
Dear Ms. Sykes:
. . . Since you had MMI's alleged employment letter from the start of this investigation, and you nevertheless investigated DCI . . . without any complaint being issued against MMI, we believe that this subpoena is a lame effort to cover up your own mistake. Your unprofessional conduct toward counsel for the Respondent supports this hypothesis. You have lost all objectivity, and you have no business remaining on this case. Any effort to enforce this subpoena would be absurd, but if you do so, we look forward to the opportunity of deposing you, and giving you a taste of your own medicine.
In response to this aggressive and hostile tone, Sykes phoned Walters. "These are very evil people," she told her. "I can't give you any advice except that you need to pray for them."
Cohen aimed his fire at Walters as well. In an April 1995 letter, he warned her that she had seven days to withdraw her complaint, or they would pursue action against her personally for malicious prosecution, or abuse of process. This threat came at a particularly vulnerable time for Walters. Tensions were running high at home. Steve's job at the Environmental Protection Agency was on shaky ground because of layoffs. Again Steve asked Margaret to put an end to the legal battle -- whatever that entailed.
Walters spent her days following up employment leads, working mindless temp jobs and handing over her unemployment checks to Jackie and Elizabeth's day-care center. Finally the slow machinery of the Maryland commission made a finding of probable cause of pregnancy discrimination.
For every step Walters took, however, the Downeys countered. In May 1995 a late-model brown sedan pulled up in front of Walters's house. A burly off-duty police officer handed Walters a summons. As she read it, a feeling of panic swept over her. DCI was suing Walters in Virginia for abuse of process and breach of settlement. The Maryland commission had no jurisdiction in Virginia. Margaret Walters was on her own.
Alan Grayson is a Harvard Law School graduate, tall and slim, self-assured and righteous. He has been the Downeys' counsel for more than 10 years. "The whole idea of these people being sued for pregnancy discrimination was far-fetched to start with," he says. By the spring of 1995, as the case headed to the courts, Grayson personally took over the Downeys' defense. When Mark Wasserman, Walters's newly hired lawyer in Virginia, successfully sought an injunction against DCI to stop its lawsuit,Grayson refiled and an appellate court reversed the earlier ruling, allowing the Downeys' suit to go forward.
Walters and her lawyer believed the suit against her constituted illegal retaliation, and in November Walters added this charge to her Maryland complaint.
Letter from Mark Wasserman, 9/5/95:
Dear Mr. Grayson:
You continued to demonstrate your total lack of professionalism by calling me an [expletive] today. I will not tolerate that and I hung up the phone as a result, as I will in the future should you continue your abusive behavior . . .
Letter from Alan Grayson, 9/8/95:
Dear Mr. Wasserman:
I don't understand what you think you can accomplish by such snide and inexplicable remarks as, "your reputation proceeds you"* or "you continued to demonstrate a total lack of professionalism."
Rather than trying to demonize me personally in this wholly unpersuasive manner, I suggest that you give some thought as to why your client continues to harass DCI long after it was clear to her that DCI had nothing to do with any employment offer to her. Your feigned indignation, directed at me personally, is no substitute for a valid defense.
*The correct terminology is, "your reputation precedes you."
Loretta Downey, for one, was fuming, and the Downeys and Alan Grayson were now determined to take the matter to trial. While the Downeys were readying their legal arsenal for trial, Walters added a major weapon to her own.
Sue Huhta had been at Arnold & Porter for only two years. Intense and edgy, she was on the lookout for a compelling case to add to Arnold & Porter's roster. When she learned of Walters's suit, which was being shopped around by the Washington Lawyers' Committee for Civil Rights, she decided to jump in.
Paper started to fly. Arnold & Porter sent document requests to Grayson & Associates for the Downeys' files. Grayson fired back with 22 third-party subpoenas -- including to Walters's dry cleaner, her tailor, her credit card company, and her OB-GYN. By now, the case had passed from the Maryland commission into the federal jurisdiction of the EEOC. Trial was set for January 1999.
At one point, the battleground shifted to Florida, where lawyers from both sides flew to depose Pat Flannery, who had been fired from DCI in 1997. Huhta and Grayson squared off over the question of attorney-client privilege.
Deposition of Pat Flannery, 3/27/98:
Mr. Grayson: Hold it. I have something to say that's very important. I don't want you to interrupt until I'm finished. We just adjourned and Ms. Huhta, the attorney for Ms. Walters, called Mr. Flannery's attorney and spoke to her from 11:18 until 11:50. I asked to remain in the room and she refused and insisted that I leave the room and not participate in the conversation.
At some later point, Mr. Flannery rejoined them. I knocked on the door, again asked to come into the room and she again insisted that I leave the room. I surmise from this that there were material discussions regarding this case between herself and Mr. Flannery and Mr. Flannery's attorney who is an agent of Mr. Flannery . . . On the basis of her flagrant disregard for the attorney-client privilege . . . I ask Ms. Huhta and her firm to disqualify themselves from any further action in this case and leave this room.
Heated discussion and more accusations followed:
Mr. Grayson: Let the record reflect that Ms. Huhta is laughing at the prospect of her actually having to follow a Supreme Court of Maryland decision.
Grayson went on to file a motion with the court to force Arnold & Porter to withdraw. The judge refused.
Memorandum and Order by United States District Judge Frederic N. Smalkin, 5/5/98:
. . . this simple, one-plaintiff pregnancy discrimination case has now descended into an unseemly morass that approaches the intolerable.
By now there was such suspicion on both sides that when Grayson paid a visit to Arnold & Porter's offices to measure and examine Walters's interview clothes, he was closely escorted wherever he went -- even to the restroom.
In the meantime, heavy damage to the Downeys' defense came from Harvey Richmond, who was fired just three months after Walters was offered employment at MMI.
Deposition of Harvey Richmond, 3/2/98:
Q: Can you tell me what was said during your phone conversation?
A: I told her that we were sorry to inform her that we had changed the scope of the job. . . . As a result of that, we had decided to wait until our extended requirements were fully known before proceeding with the hire, and we were postponing our hiring position.
Q: Why did you tell Ms. Walters that?
A: Because Ed Downey instructed me to.
Q: Was it your belief that that was the reason you were either revoking her job offer or postponing the hiring decision.
A: Not really.
Q: What was your belief as to the reason the job offer was revoked?
A: Because she deceived us, according to Loretta Downey.
A: Do you consider the contents of this letter [sent by Richmond to Walters explaining why they could not hire her] to be truthful at the time they were written -- it was written, excuse me.
Mr. Grayson: Objection; vague. You can answer.
The Witness: They are misleading.
Richmond, who promptly joined Walters's previous employer -- the rival marketing firm Information Resources Inc. -- after he was fired, went on to state that the rescinded job never changed in the way the Downeys had suggested and that the woman who finally took the position was considerably less qualified than Walters.
Before Richmond left, however, he said, the Downeys offered him a severance package of approximately $75,000, contingent upon his signing an affidavit corroborating their version of events in the Walters case. Richmond refused to sign.
In August 1998, Judge Smalkin ruled that DCI/MMI constituted a single integrated employer. Walters, it appeared, hadn't sued the wrong company after all. Smalkin also found ample evidence of pregnancy discrimination. Further, he agreed that the plaintiffs had established a sound basis for charging the Downeys with retaliation. He denied the Downeys' assertion that Walters breached the settlement agreement and called their claim that Walters fraudulently backdated her amended charge "patently ridiculous."
The Downeys had lost on all fronts. In desperation, they switched legal horses, hiring the Baltimore firm Hogan & Hartson, which specializes in employment law. Gil Abramson, who was now handling their case, spent the next few months stepping gingerly around veritable land mines left behind from four years of bitter litigation.
Although Abramson concluded his clients would have had a good chance in court, the Downeys decided to settle. The sheer cost of bringing the case before a jury -- an amount well into six figures -- persuaded them to quit. "It was a business decision," says Abramson. They also feared that if Walters won, Arnold & Porter would demand attorneys fees -- another six-figure sum.
Under the negotiated settlement the Downeys agreed to pay Walters $95,000, $13,000 of which would go to partially reimburse her legal fees. Walters would eventually go home with about $60,000. In addition, the EEOC would closely monitor DCI/MMI hiring and employment practices over the next 18 months.
While the case had officially come to an end, the caustic residue would remain for some time to come. "If there was some way I could have reached a more fair outcome, I would have done it," says Alan Grayson. "There should have been a clear-cut win for the Downeys."
Sue Huhta, of course, sees it much differently. "The tactics we were faced with presented difficult challenges," she says. "I have nothing short of pride regarding our responses." The Walters case was one of several cited when Arnold & Porter was named D.C.'s 1999 Pro Bono Law Firm of the Year.
One of the springer spaniels ambles into Loretta Downey's office and flops down next to her desk. There is the sound of light laughter from an adjoining office and the smell of coffee brewing. On a wall, as ordered by the EEOC, is a posted notice announcing the outcome of the lawsuit, and DCI/MMI now has a human resources expert to keep them out of trouble.
To this day Loretta Downey and Margaret Walters have never met nor spoken. But Downey, her cancer now in remission, has her own sense of Walters's motivations. "I would guess she saw this as an opportunity to make some money. I try to think of another scenario and I can't really. Ed said `shakedown.' I don't think that's too strong a term."
Walters, who gave birth to another girl, Caroline, in the summer of 1998, feels deeply grateful for Arnold & Porter's commitment to her case -- as well as vindicated. What DCI/MMI did was "illegal," she says. "It was my obligation to pursue it."
As it turned out, resolution came at a critical moment for Walters. During final settlement negotiations with the Downeys, Jackie was diagnosed with leukemia. The money from the settlement has helped the family cover expenses during her treatment.
Asked if she would go through this kind of legal ordeal again, Walters considers the question for a moment. "I guess I'd say I would, because I can't imagine that this bizarre thing could ever happen again."
Letter from Ed Downey to Fred Cohen, 1/18/95:
Fred: The attached [subpoena] is a real pain in the ass because of the amount of work it will require plus the fact that most of it is pure nonsense and ridiculous.
Let me know what you think.
Ed.
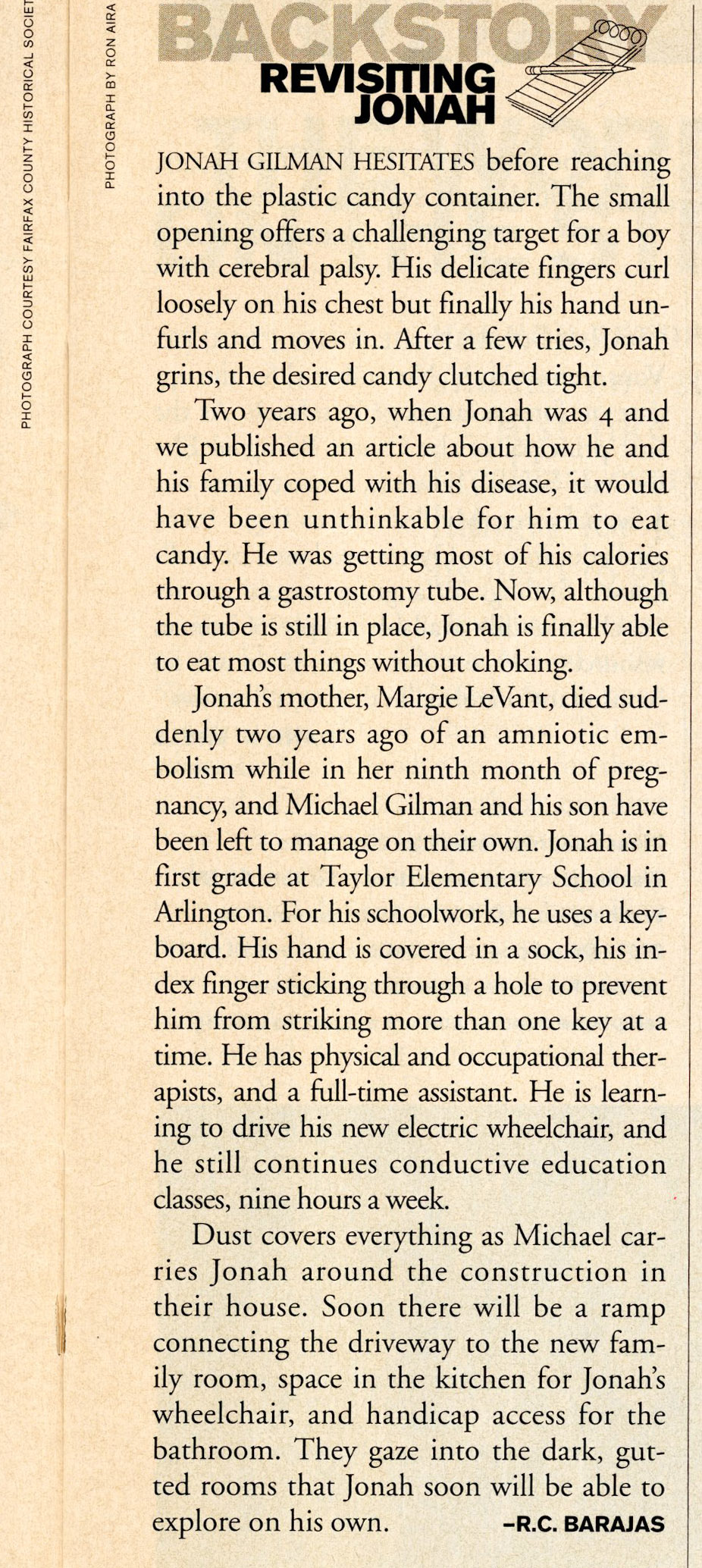
R.C. Barajas last wrote for the Magazine about a boy with cerebral palsy and his mother.
 R. C. Barajas
R. C. Barajas